Understanding Testosterone Deficiency
A comprehensive guide to primary hypogonadism, age-related testosterone decline ("manopause"), and how Testosterone Replacement Therapy can help restore quality of life.
What is Testosterone?
Testosterone is the primary male sex hormone and anabolic steroid. It plays a critical role in the development of male reproductive tissues and promotes secondary sexual characteristics such as increased muscle and bone mass, and the growth of body hair.
Beyond its role in reproduction, testosterone is vital for overall health and well-being. It influences mood, energy levels, cognitive function, cardiovascular health, and body composition throughout a man's life.
Testosterone is produced primarily in the testes, regulated by a complex feedback loop known as the Hypothalamic-Pituitary-Gonadal (HPG) axis.
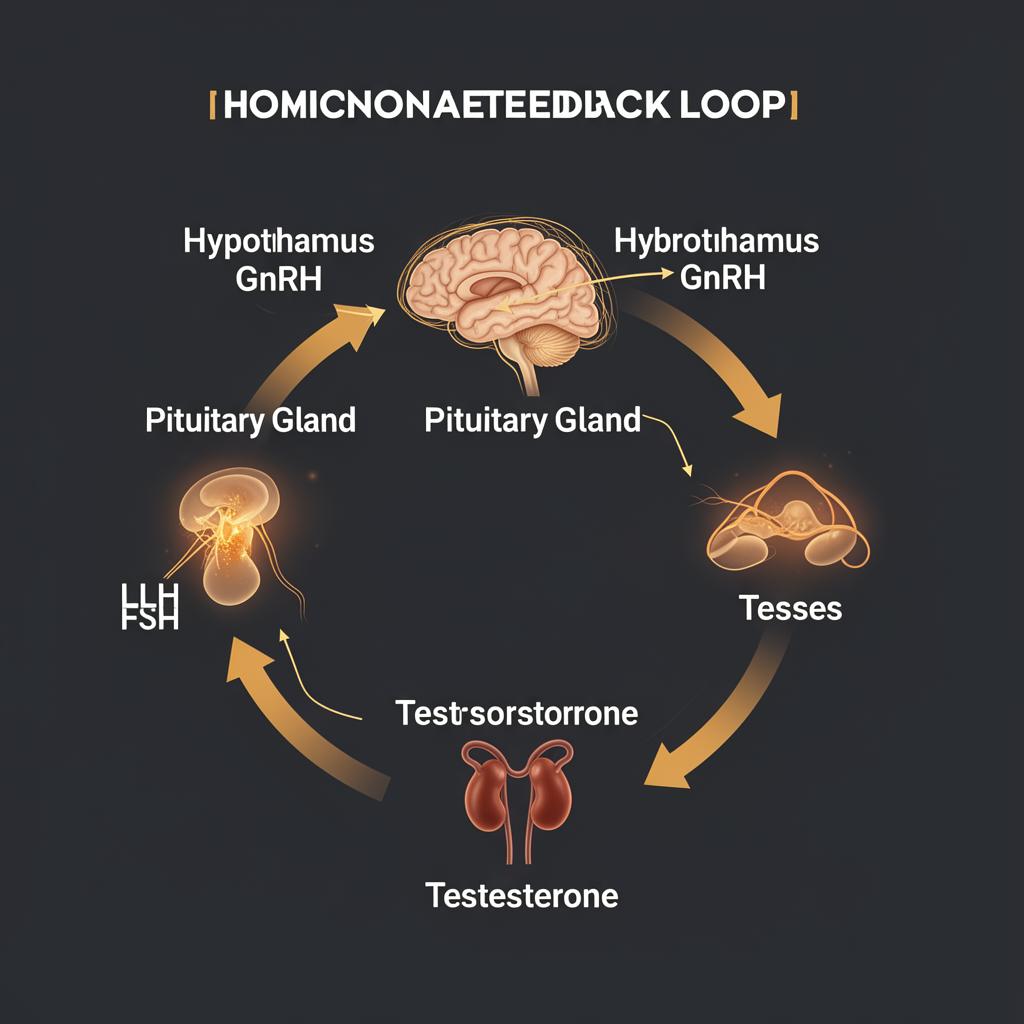
The HPG Axis — Hormonal Feedback Loop
The HPG Axis Explained
Hypothalamus
The hypothalamus releases Gonadotropin-Releasing Hormone (GnRH) in a pulsatile fashion, signalling the pituitary gland to produce gonadotropins.
Pituitary Gland
In response to GnRH, the anterior pituitary releases Luteinising Hormone (LH) and Follicle-Stimulating Hormone (FSH) into the bloodstream.
Testes (Leydig Cells)
LH stimulates the Leydig cells in the testes to produce testosterone. FSH supports spermatogenesis. Testosterone feeds back to the hypothalamus and pituitary to regulate production.
Primary Hypogonadism
Primary hypogonadism (also called hypergonadotropic hypogonadism) occurs when the testes themselves fail to produce adequate testosterone, despite receiving appropriate signals from the pituitary gland.
In this condition, LH and FSH levels are typically elevated — the brain is "shouting louder" at the testes to produce testosterone, but the testes cannot respond adequately.
Common Causes
- Klinefelter syndrome (47,XXY)
- Undescended testes (cryptorchidism)
- Testicular injury or trauma
- Orchitis (infection/inflammation of the testes)
- Cancer treatment (chemotherapy or radiation)
- Mumps orchitis
- Haemochromatosis (iron overload)
Primary vs Secondary Hypogonadism
Primary (Testicular Failure)
Low testosterone + High LH/FSH
The problem originates in the testes
Secondary (Central/Pituitary)
Low testosterone + Low/Normal LH/FSH
The problem originates in the hypothalamus or pituitary
Key Diagnostic Markers
- Total testosterone (morning sample)
- Free testosterone / SHBG
- LH and FSH levels
- Prolactin
- Oestradiol (E2)
- Full blood count (haematocrit)
- PSA (prostate-specific antigen)
- Metabolic panel and lipids
Age-Related Decline in Total Testosterone
Estimated mean total testosterone (ng/dL) by age
Modelled on data from Feldman et al. (2002) — ~1.6% annual decline in total testosterone.
Red dashed line indicates the clinical threshold for testosterone deficiency (~300 ng/dL).
"Manopause" — Male Andropause
Unlike female menopause, which involves a relatively abrupt decline in hormones, andropause (commonly called "manopause" or "male menopause") is characterised by a gradual, progressive decline in testosterone levels.
The landmark Massachusetts Male Aging Study (MMAS) — a large population-based prospective study — demonstrated that total testosterone declines at a rate of approximately1.6% per year, while free and albumin-bound testosterone decline even more steeply at 2–3% per year (Feldman et al., 2002).
This age-related decline is now recognised as Late-Onset Hypogonadism (LOH) — a legitimate clinical condition that can profoundly impact quality of life, physical health, and mental well-being. The MMAS data showed that by age 70, the average man's total testosterone has fallen to roughly half of peak levels.
It's important to note that not all men will experience symptomatic testosterone deficiency — lifestyle factors including sleep, exercise, stress management, and body composition play a significant role in testosterone levels.
Signs & Symptoms
Low testosterone can manifest across physical, psychological, and sexual domains. Symptoms are often gradual and may be attributed to "normal ageing."
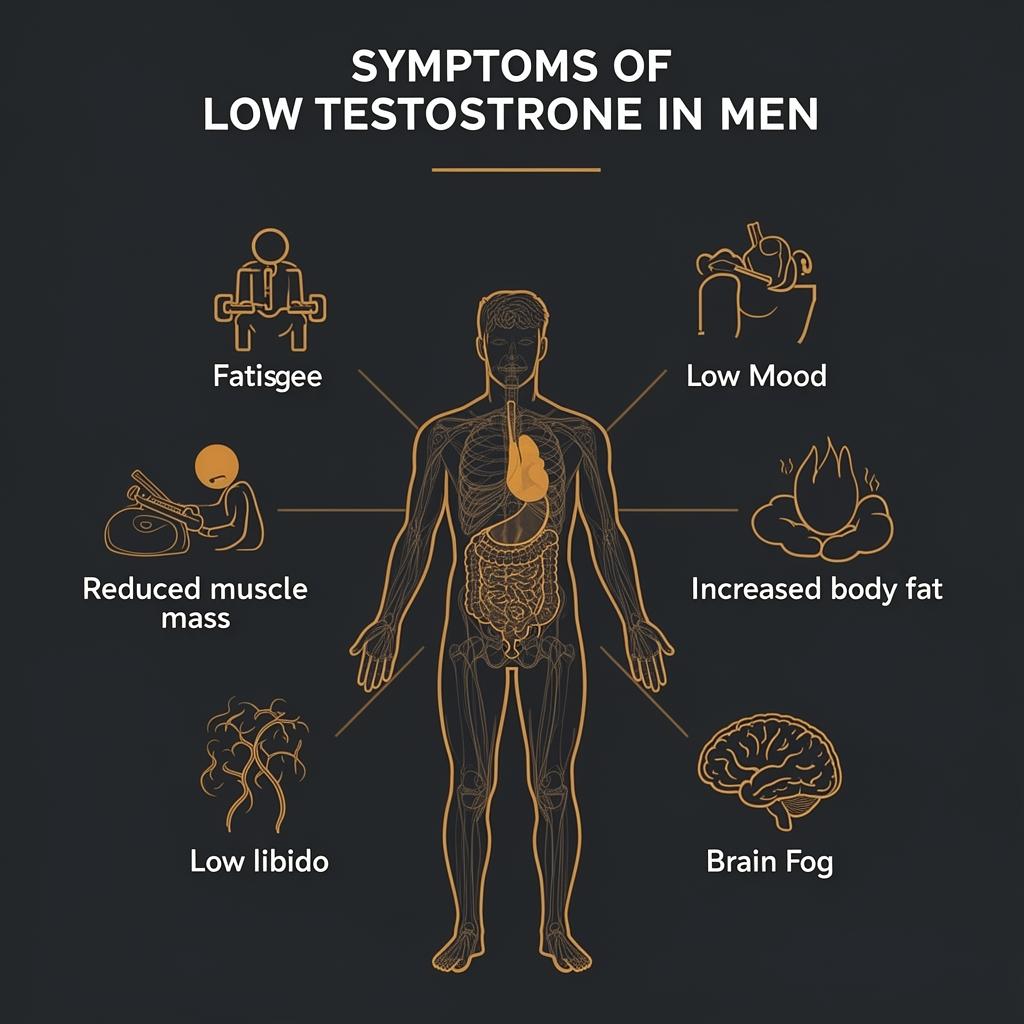
Physical
- Decreased muscle mass and strength
- Increased body fat (especially visceral)
- Reduced bone mineral density
- Fatigue and reduced stamina
- Hot flushes and night sweats
Psychological
- Low mood and irritability
- Brain fog and poor concentration
- Reduced motivation and drive
- Anxiety and depressive symptoms
- Sleep disturbances
Sexual
- Reduced libido
- Erectile dysfunction
- Decreased morning erections
- Reduced fertility / sperm count
Metabolic
- Insulin resistance
- Dyslipidaemia
- Increased cardiovascular risk markers
- Anaemia
Treatment Options
Testosterone Replacement Therapy aims to restore testosterone levels to the physiological range, alleviating symptoms and improving quality of life. Several delivery methods exist — but not all are equal.
Intramuscular Injection (IM)
Intramuscular testosterone injection — typically Testosterone Cypionate or Enanthate — is widely regarded as the gold standard of TRT delivery. Here's why:
- Proven efficacy: Decades of clinical data and the most extensively studied delivery method in TRT literature.
- Reliable absorption: Deposited directly into muscle tissue, ensuring predictable and consistent pharmacokinetics with every dose.
- Dosing flexibility: Titrated tailored to patient's needs — frequency can range from daily to fortnightly depending on ester and individual response.
- Full PHARMAC subsidy: For those who meet primary hypogonadism diagnosis criteria, injectable testosterone is fully funded under PHARMAC.
- No transference risk: Unlike topical formulations, there is zero risk of transferring testosterone to partners, children, or pets through skin contact.
- Measurable peak and trough: Blood levels can be accurately timed and measured, allowing precise dose optimisation by your clinician.
- Self-administration: Patients can be trained to self-inject at home, reducing the need for frequent clinic visits.
At Enhanced TRT, intramuscular injection is our primary recommended protocol. We use pharmaceutical-grade Testosterone Cypionate with individualised dosing schedules to achieve optimal, stable serum levels.
Other Delivery Methods
Topical Gels & Creams
Applied daily to the skin. Can provide steady-state levels but requires strict daily compliance, has variable absorption rates (especially with sweating or showering), and carries a significant risk of transference to others via skin contact.
Subcutaneous Injections
Lower-volume, more frequent injections using smaller needles into fatty tissue. May suit patients who prefer smaller needles, though absorption can be less predictable than intramuscular delivery.
Transdermal Patches
Worn on the skin daily. Often cause local skin irritation and adhesion issues. Absorption varies widely between individuals and is affected by body hair and perspiration.
Testosterone Pellets (Implants)
Surgically implanted subcutaneously every 3–6 months. Provide long-acting release but require a minor procedure, carry infection risk, and dosing cannot be easily adjusted once implanted.

Common TRT delivery methods
Ongoing Monitoring
Safe TRT requires regular blood work and clinical review to ensure optimal outcomes and minimise risks.
Testosterone Levels
Total and free testosterone to ensure therapeutic range
Haematocrit / Hb
Monitor for polycythaemia (elevated red blood cells)
PSA
Prostate-specific antigen screening for prostate safety
Oestradiol
Monitor oestrogen conversion and manage side effects
Liver Function
Hepatic markers to assess metabolic impact
Lipid Profile
Cholesterol and triglyceride monitoring
Mood & Symptoms
Subjective well-being, libido, energy assessment
Cardiovascular
Blood pressure, heart rate, and risk factor assessment
Risks & Considerations
Potential Side Effects
- Polycythaemia (elevated haematocrit) — requires monitoring
- Acne and oily skin
- Mood changes or irritability (especially with supraphysiologic levels)
- Testicular atrophy and reduced fertility
- Oestrogen-related effects (gynaecomastia, water retention)
- Sleep apnoea exacerbation
- Potential cardiovascular considerations (ongoing research)
Important Considerations
- TRT suppresses natural testosterone production and spermatogenesis
- Fertility preservation should be discussed before starting TRT
- HCG may be co-prescribed to maintain testicular function
- Lifestyle optimisation (sleep, exercise, diet, stress) should be addressed first
- Regular follow-up is essential — TRT is not a 'set and forget' treatment
- Blood donation may be required if haematocrit rises
- TRT is a long-term commitment in most cases
Think You May Have Low Testosterone?
Start with our free Aging Males' Symptoms questionnaire to assess your risk, or book a confidential telehealth consultation.